
Disorganized attachment is a pattern that forms when a child's caregiver is simultaneously their source of safety and their source of fear—what researchers call "fright without solution" (Main and Hesse, 1999). Infants whose parents displayed frightened, frightening, or dissociative behavior were 3.7 times more likely to develop disorganized attachment (Duschinsky, 2018). This pattern affects approximately 15 percent of the general population and up to 80 percent of children in maltreated samples (Pollard et al., 2023).
If you have disorganized attachment and feel like healing is slower or more confusing than what you read about online, you are not imagining it. Research confirms this style involves unique neurobiological, dissociative, and relational barriers that other insecure styles do not carry. This article names those barriers—so that what you're experiencing starts to make sense, not so you can fix it on a timeline.
Key takeaway: Disorganized attachment is harder to heal than other insecure styles because it creates a biological paradox where closeness equals danger, stores trauma in implicit body-based memory that talk therapy alone cannot reach, and triggers the same approach-avoid conflict inside the healing relationship itself. Recovery is possible but requires phase-based treatment typically exceeding 16 sessions.
What Makes Disorganized Attachment Different from Other Insecure Styles?
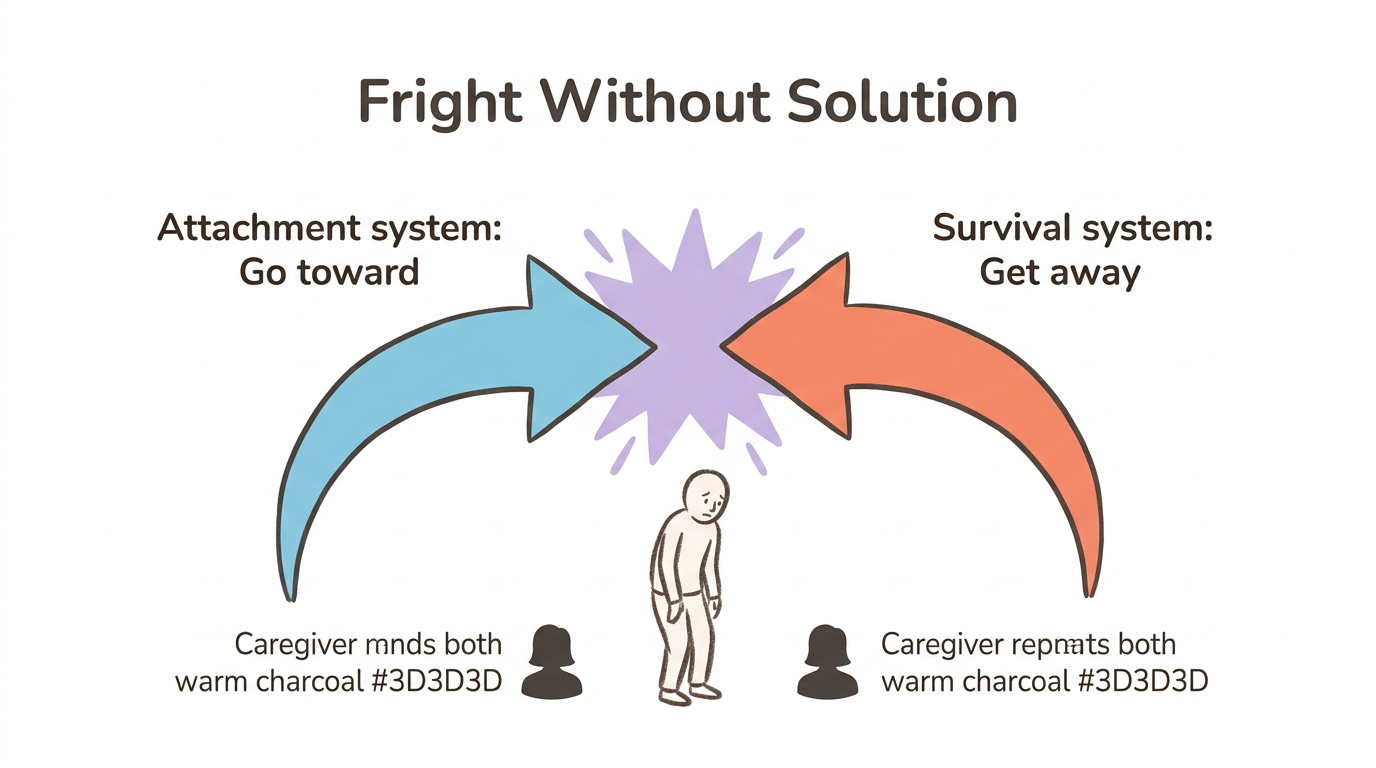
Disorganized attachment is the only insecure style that lacks a coherent strategy for managing distress. Anxious attachment hyperactivates the attachment system—reaching, protesting, clinging. Avoidant attachment deactivates it—withdrawing, numbing, self-relying. Both are organized responses. Disorganized attachment has no single strategy because the child's nervous system receives two contradictory commands at once.
This is the "fright without solution" paradox. Every mammalian infant is biologically driven to seek their caregiver when afraid. But when the caregiver is the source of fear—through frightened expressions, threatening behavior, or dissociative absence—the child cannot approach or flee. Their attachment system says go toward. Their survival system says get away. Neither wins. The result is the simultaneous activation and collapse you may recognize in yourself: wanting closeness desperately while feeling terrified of it.
A meta-analysis of more than 20,000 infant-parent dyads found that 23.5 percent of children showed disorganized attachment (Van IJzendoorn et al.). For a full overview of how this pattern develops, see What Is Disorganized Attachment and How Does It Affect Relationships?. The approach-avoid conflict at the core of disorganized attachment is not a choice or a personality flaw. It is your nervous system running two survival programs simultaneously—a legacy of circumstances that were never your fault.
Map Your Contradictory Impulses (for disorganized attachment)
When opposing impulses stay unconscious, they create freeze or chaos. This exercise externalizes the internal contradiction so you can observe it rather than collapse into it.
- Notice when you feel pulled in two directions during a relational moment—wanting to reach out but also wanting to disappear
- Open a journal or notes app and draw two columns: "Part of me wants to..." and "But another part wants to..."
- Fill both columns without editing or judging what appears
- Read both columns aloud, starting each with "A part of me..."
- Notice what shifts in your body when both impulses are acknowledged rather than fought
Naming both sides builds the observer awareness that disorganized attachment disrupts—the capacity to witness your experience without being consumed by it.
How Does Disorganized Attachment Change the Brain?
Research by Arancibia et al. (2023) identified measurable changes in brain structure and stress physiology among people with disorganized attachment histories—though the authors emphasize that available evidence still comes from small samples and lacks the robustness for clinical application.
Here are the four key brain regions affected and what each means for daily life:
- Amygdala—Adults who were classified as disorganized in infancy show an enlarged left amygdala, the brain's threat detection center. This translates to hypervigilance in relationships: scanning for danger in a partner's tone, expression, or silence.
- Hippocampus—Mixed findings show altered hippocampal volume and functional connectivity, which may contribute to fragmented memory encoding. Emotional experiences feel disconnected from their context, as if pieces of the story are missing.
- Prefrontal cortex and anterior cingulate cortex—Altered activation during attachment-related tasks impairs top-down emotional regulation. When your threat system fires, the brain regions responsible for calming it down respond more slowly.
- Insular cortex—Changes in interoceptive processing make it harder to read your own body signals. You may struggle to distinguish hunger from anxiety, exhaustion from sadness, or genuine intuition from activation.
Beyond brain structure, disorganized attachment disrupts the stress hormone system. Infants with disorganized attachment show flattened diurnal cortisol slopes—their stress response does not properly ramp up in the morning or wind down at night (Arancibia et al., 2023). The oxytocin system is also affected: disorganized individuals show suppressed bonding-hormone responses under stress, meaning the neurochemical system designed to make closeness feel safe does not activate when needed most.
One finding offers relief: the genetic contribution to disorganized attachment is approximately zero (Arancibia et al., 2023). This pattern is not hardwired into your DNA. It was shaped by experience—and experience-dependent changes in the brain can be reshaped through new relational experiences. For more on how attachment shapes your nervous system, see How Does Attachment Style Affect Your Nervous System?.
Why Does Talk Therapy Alone Often Fall Short?
If you have been in therapy and felt like something was not quite landing, there is a neurobiological reason. The trauma in disorganized attachment is stored in implicit memory—non-conscious, body-based patterns—rather than in the narrative memory that conversation accesses. Your body holds the terror, the freeze, and the collapse as procedural responses that activate without any conscious story attached to them.
Explicit memory is what you can describe: "My father used to yell." Implicit memory is what your body does when someone raises their voice—the stomach drop, the dissociation, the sudden blankness. You experience the full physiological response without understanding why it is happening. Research on implicit memory in trauma-related disorders confirms that healing requires modification of these non-conscious patterns, not just conscious elaboration of autobiographical memories (PMC11523743).
The longitudinal evidence underscores how deep these patterns run. The correlation between degree of disorganization in infancy and psychiatric symptoms at age 17.5 approaches r = .40 (Sroufe et al.)—a remarkably strong relationship spanning nearly two decades. Your body remembers what the mind can't narrate, and cognitive insight alone cannot overwrite what the nervous system encoded before you had words.
Your nervous system learned these procedural patterns for survival. They were adaptive once—your body found the best available response to an impossible situation. Recognizing that talk therapy alone may not reach them is not a failure. It is information that points you toward body-inclusive approaches that can.
The 5-4-3-2-1 Grounding Anchor (somatic technique for disorganized attachment)
- When you notice dissociation, freeze, or a sudden sense of "leaving your body," pause wherever you are
- Name 5 things you can see—say them aloud or silently
- Touch 4 different surfaces and notice their texture
- Identify 3 sounds in your environment
- Notice 2 things you can smell
- Name 1 thing you can taste
- Place one hand on your chest and one on your belly. Take 3 slow breaths, feeling the warmth of your hands
This engages the ventral vagal system through sensory orientation, interrupting the dorsal vagal shutdown that disorganized attachment activates when implicit memory is triggered. Bringing attention to the five senses pulls your nervous system back into the present moment—the opposite of the dissociative collapse where past and present blur together. For more on this mechanism, see What Is the Window of Tolerance?.
Why Does the Healing Relationship Itself Feel Threatening?
You might expect a safe therapeutic relationship to feel like relief. For disorganized attachment, it often feels like a threat—because your brain has learned to read closeness as danger. A therapist offering safety, attunement, and consistent presence activates the same biological paradox that the original caregiver created: approach the person who might hurt you, or flee the person who might help you.
This is what clinicians call the therapeutic paradox. The very conditions required for healing—trust, vulnerability, being seen—are the exact conditions your nervous system learned to flag as threats. Your body does not distinguish between a caregiver who was frightening and a therapist who is safe. It runs the same survival program: rapid cycling between sympathetic hyperarousal and dorsal vagal collapse (Porges). Liotti (2019) described how this process fragments the sense of self through structural dissociation—you are not one person resisting help, but multiple self-states with contradictory goals.
That urge to cancel your next session, the sudden conviction that your therapist does not actually care, the blankness that descends mid-conversation—these are not signs of failure. Wanting to quit therapy is the pattern, not the problem. Your attachment system is doing exactly what it was trained to do. If you recognize the push-pull dynamic in your therapeutic relationship, that is actually a sign that meaningful attachment work is happening.
Name the Part, Not the Whole (IFS-informed, for disorganized attachment)
Disorganized attachment tends to produce all-or-nothing responses—total withdrawal or total collapse. This exercise creates distance between a protective impulse and the whole self, interrupting what Liotti (2019) describes as structural dissociation.
- When you notice yourself wanting to flee a therapy session, a conversation, or a relationship, pause
- Say internally: "A part of me wants to leave right now"
- Ask that part: "What are you afraid will happen if I stay?"
- Write down whatever answer comes—without censoring or analyzing
- Then ask: "How old does this part feel?"
- Thank the part for trying to protect you
Over time, naming "a part" rather than identifying with the entire impulse builds the self-observer capacity that disorganized attachment disrupts.
Are There Different Types of Adult Disorganized Attachment?
Yes—research identifies at least two distinct subtypes that require different treatment approaches. A latent class analysis by Levy et al. (2015) studying 272 adults found two disorganized profiles, each with different presentations and different healing needs.
Disorganized-Oscillating (28 percent of the sample)
This subtype shows elevated BPD severity, identity disturbance, and poor self-other differentiation. If this is your pattern, you may experience intense emotional swings—rage followed by desperate longing, idealization followed by devaluation. Disorganized-Oscillating presentations often involve what feels like an unstable sense of who you are, particularly in close relationships. Research shows 66 percent of BPD patients experience pathological dissociation (BPD Foundation), and up to 56 percent of people with BPD also meet criteria for PTSD (Frontiers, 2018).
Disorganized-Impoverished (19 percent of the sample)
This subtype shows highest avoidant and schizoid scores, severe mentalization difficulties, and lower affective intensity. If this resonates, you may feel emotionally flat rather than chaotic—struggling to access feelings at all, experiencing relationships as confusing or pointless, feeling numb when closeness is offered. Disorganized-Impoverished presentations need affect-building and mentalization training rather than emotion regulation work.
Both subtypes showed significantly worse personality functioning, work dysfunction, relationship difficulties, and hostility (Levy et al., 2015). Different subtypes need different treatment. Generic attachment advice that does not distinguish between oscillating and impoverished patterns may miss what you actually need.
Subtype Self-Reflection (for both disorganized subtypes)
- Read through these two columns of descriptors:
- Oscillating: intense emotional swings, identity confusion, idealizing then devaluing, fear of abandonment, impulsive under stress
- Impoverished: emotional flatness, difficulty naming feelings, withdrawal from relationships, confusion about what you want, feeling like an observer of your own life
- Without forcing a choice, notice which column produces more body recognition—a tightening, a familiar feeling, or a quiet "yes"
- Write down 2-3 specific situations where you recognized your pattern from that column
- Bring this reflection to your next therapy session as a conversation starter
This is not a diagnosis—it is a starting point. Many people with disorganized attachment receive generic advice that misses their specific pattern. Recognizing whether you tend toward oscillating or impoverished responses helps you and your therapist target treatment more precisely, rather than applying approaches designed for the opposite subtype.
Why Does Healing Disorganized Attachment Take Longer?
Multiple compounding barriers—not a single obstacle—explain the longer timeline. Meta-analytic evidence confirms that interventions need more than 16 sessions to produce significant improvement. Fewer than 15 sessions show no meaningful change (Wright and Edginton, 2016).
The intervention research reveals a counterintuitive finding. Sensitivity-focused interventions alone (effect size d = 0.24) significantly outperformed broader interventions that also included support and mental representations work (d = -0.04) (Bakermans-Kranenburg et al., 2017). The overall effect size for reducing disorganized attachment was d = 0.35. Simpler, focused approaches appear to work better than comprehensive but diffuse ones—though all approaches require sustained engagement over time.
Comorbidity compounds the timeline. Disorganized attachment rarely exists in isolation. The overlap with BPD, PTSD, and dissociative disorders means treatment must address multiple interlocking conditions. Each comorbidity adds complexity and extends the path. The dissociative component is particularly challenging: you cannot process what you cannot stay present for.
The path from disorganized to earned secure attachment is longer and more non-linear than from anxious or avoidant styles, primarily because of these dissociative and trauma components. But earned security is achievable. Roisman et al. (2002) found that people who earned secure status parent as effectively as those who were continuously secure throughout their lives. The destination is the same—the route is longer.
You did not choose the longer path. Your nervous system was handed a more complex map. Recognizing that healing takes longer is not pessimism—it is the realistic expectation that prevents you from abandoning the process when progress feels slow. The meta-analytic data suggests progress is measurable in smaller increments—noticing activation slightly earlier, responding slightly differently, slightly more often.
Window of Tolerance Tracking (for disorganized attachment)
The insular cortex changes identified by Arancibia et al. (2023) make it genuinely harder to read your own body signals. This tracking practice creates external data for what your internal compass struggles to register.
- Set 3 gentle alarms throughout your day—morning, midday, evening
- At each alarm, check in: Am I in hyperarousal (racing heart, anxiety, anger, restlessness)? Hypoarousal (numb, foggy, collapsed, disconnected)? Or within my window (present, able to think and feel simultaneously)?
- Record your state with a single word or symbol in your phone's notes
- At the end of one week, review the pattern: What time of day are you most often outside your window? What preceded the shifts?
- Share this data with your therapist
Over time, this practice expands your window of tolerance by building the foundation for noticing shifts before they become full nervous system collapse.
What Treatment Approaches Actually Work?
Phase-based treatment is the gold standard for disorganized attachment, supported by consensus across leading trauma researchers (Van der Hart, Nijenhuis, Fisher, Siegel). Trying to process trauma before your nervous system can tolerate the activation leads to retraumatization, not healing.
The three phases of treatment:
- Stabilization—Building safety, learning nervous system regulation, and developing the therapeutic relationship. This phase may take months before any direct trauma work begins, and it is not wasted time. It is the foundation everything else depends on.
- Processing—Working through traumatic material using approaches that access implicit memory: EMDR targets body-stored trauma through bilateral stimulation, IFS works directly with the fragmented self-states that disorganized attachment creates, and Somatic Experiencing addresses freeze and collapse responses that talk therapy cannot reach.
- Integration—Reconnecting with relationships, building earned security, and consolidating new relational patterns into daily life.
No single modality is sufficient for most people with disorganized attachment. The dissociative component may need IFS or parts work. The body-level activation may need somatic approaches. The relational patterns may need attachment-focused therapy. Research on security priming—repeated exposure to secure attachment imagery—shows promise for modifying the internal working models that maintain disorganized patterns, including reductions in dissociation (PMC11523743).
For a detailed comparison of specific therapeutic modalities, see What Therapy Is Best for Disorganized Attachment?. The most important factor is finding a therapist trained in complex trauma who understands why your nervous system treats the healing relationship as a threat—and has the patience to work with that rather than against it.
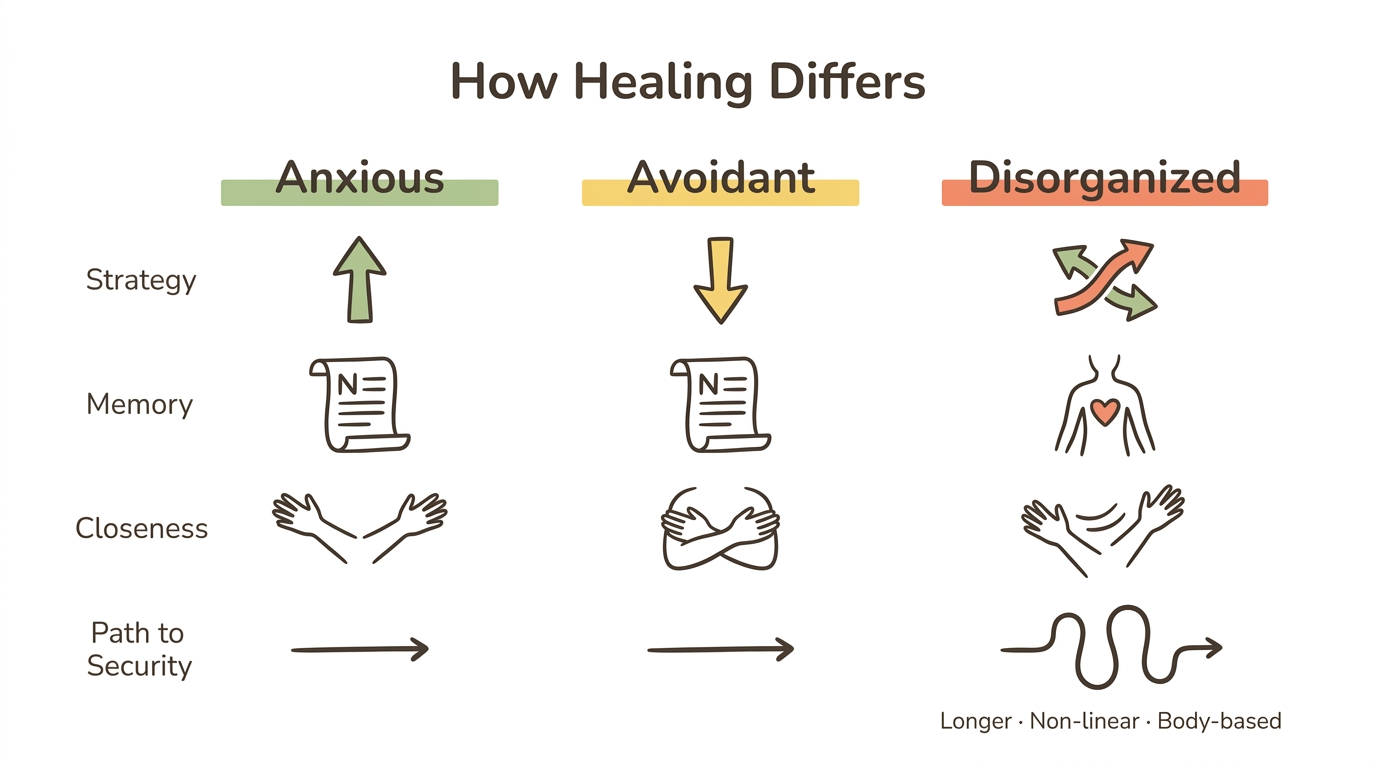
How Does Healing Differ Across Attachment Styles?
| Anxious | Avoidant | Disorganized | |
|---|---|---|---|
| Core challenge | Hyperactivation of attachment system | Deactivation of attachment system | No coherent strategy—simultaneous activation and deactivation |
| Where trauma is stored | Primarily explicit and narrative memory | Primarily explicit and narrative memory | Primarily implicit and body-based memory |
| Response to therapeutic closeness | Seeks it, sometimes excessively | Resists it, deactivates | Paradox: seeks AND fears it simultaneously |
| Typical sessions for progress | 12-16 sessions | 16-20 sessions | More than 16 sessions minimum, often 1-2 years or longer |
| Dissociation risk | Low | Low to moderate | High |
| Comorbidity burden | Anxiety, depression | Depression, emotional suppression | BPD, PTSD, dissociative disorders |
| Primary treatment focus | Emotion regulation and self-soothing | Affect tolerance and vulnerability | Phase-based: stabilize, process, integrate |
| Path to earned security | Shorter, more linear | Moderate, requires vulnerability practice | Longer, non-linear, requires body-based work |
When Should You Seek Professional Support?
Self-help has limits with disorganized attachment. While the exercises in this article can build awareness and offer moments of regulation, disorganized attachment almost always requires professional support—particularly when dissociation, trauma responses, or comorbid conditions are present.
Seek a complex trauma specialist if you experience any of the following: dissociative episodes where you lose time or feel detached from reality, rapid cycling between emotional extremes and numbness, difficulty maintaining any close relationship despite genuinely wanting connection, or a pattern of starting and abandoning therapy. If reading this article itself triggered a strong physiological response—tightness in your chest, a sudden urge to stop reading, a sense of fogginess—that is information worth bringing to a professional.
Look for therapists trained in EMDR, IFS, Somatic Experiencing, or Sensorimotor Psychotherapy. Ask specifically about their experience with complex trauma and disorganized attachment. The Meadow app can complement professional treatment by helping you track your patterns and practice regulation between sessions—but it is not a replacement for the relational healing that disorganized attachment requires.
Frequently Asked Questions
Can disorganized attachment be healed?
Yes. Research on earned secure attachment confirms people with disorganized histories can develop secure functioning. It typically requires phase-based treatment exceeding 16 sessions, often combining talk therapy with body-based approaches like EMDR or somatic experiencing to address implicit memory.
How long does it take to heal disorganized attachment?
Meta-analyses show interventions under 15 sessions produce no significant improvement for disorganized attachment (Wright and Edginton, 2016). Most clinicians report meaningful progress within one to two years of consistent, phase-based therapy. The timeline varies based on trauma severity, comorbidities, and the quality of the therapeutic relationship.
Can you have disorganized attachment without trauma?
Disorganized attachment requires some form of frightened, frightening, or dissociative caregiver behavior—but this does not always look like overt abuse. Subtle parental fear, unresolved grief, or emotional absence during critical moments can create disorganized patterns. Arancibia et al. (2023) found the genetic contribution to disorganized attachment is approximately zero, confirming it is experience-dependent.
Can disorganized attachment cause dissociation?
Yes. Longitudinal research shows disorganized attachment in infancy strongly predicts dissociative symptoms through childhood and into adulthood, even without additional later trauma (Liotti, 2019). The correlation between infant disorganization and psychiatric symptoms at age 17.5 approaches r = .40 (Sroufe et al.).
Is disorganized attachment the worst attachment style?
"Worst" is not clinically useful, but disorganized attachment does carry the highest risk for psychiatric comorbidities including BPD, PTSD, and dissociative disorders. It is harder to treat because it involves implicit memory, dissociation, and the therapeutic paradox where closeness triggers the same fear it is meant to resolve. However, earned security is achievable with appropriate treatment.
Why do I feel numb in relationships?
Emotional numbness in relationships often reflects dorsal vagal shutdown—a nervous system survival response common in disorganized attachment. When closeness triggers your brain's threat system, your body may collapse into freeze or dissociation rather than fight or flight. This is a protective mechanism, not a character flaw. Your nervous system learned that disappearing was safer than staying present.
Is disorganized attachment linked to BPD?
Research shows significant overlap, particularly with the Disorganized-Oscillating subtype. Up to 56 percent of people with BPD also meet criteria for PTSD, and 66 percent of BPD patients experience pathological dissociation. Some researchers conceptualize BPD as a generalization of disorganized attachment into adult personality functioning (Frontiers, 2018).
What is the difference between disorganized and fearful-avoidant attachment?
They describe the same underlying pattern using different terminology. "Disorganized" comes from developmental research using infant Strange Situation studies, while "fearful-avoidant" comes from adult attachment self-report measures (Bartholomew and Horowitz, 1991). Both describe the simultaneous desire for and fear of closeness that defines this attachment pattern.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Foundational Works
-
Main, M., & Hesse, E. (1999). Second-generation effects of unresolved trauma in nonmaltreating parents: Dissociated, frightened, and threatening parental behavior. Psychoanalytic Inquiry, 19(4), 481–540.
-
Duschinsky, R. (2018). Disorganization, fear and attachment: Working towards clarification. Infant Mental Health Journal, 39(1), 17–29. https://pmc.ncbi.nlm.nih.gov/articles/PMC5817243/
-
Van IJzendoorn, M. H., Schuengel, C., & Bakermans-Kranenburg, M. J. (1999). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11(2), 225–250.
-
Sroufe, L. A., Egeland, B., Carlson, E. A., & Collins, W. A. (2005). The Development of the Person: The Minnesota Study of Risk and Adaptation from Birth to Adulthood. Guilford Press.
Adult Classification and Subtypes
-
Levy, K. N., Johnson, B. N., Clouthier, T. L., Scala, J. W., & Temes, C. M. (2015). An attachment theoretical framework for personality disorders. Canadian Psychology, 56(2), 197–207. https://pmc.ncbi.nlm.nih.gov/articles/PMC5026862/
-
Pollard, R., Valikhani, A., & Sauer-Zavala, S. (2023). A systematic review of adult disorganized attachment measures. British Journal of Clinical Psychology, 62(2), 261–280. https://bpspsychub.onlinelibrary.wiley.com/doi/full/10.1111/bjc.12411
Neuroscience
- Arancibia, M., Ruiz, P., Casanova, J., & Sotomayor, C. (2023). Neurobiology of disorganized attachment: A review of primary studies. Neuroscience Insights, 18. https://pmc.ncbi.nlm.nih.gov/articles/PMC9947683/
Dissociation and Memory
-
Liotti, G. (2019). The role of attachment trauma and disintegrative pathogenic processes in the development of psychopathology. Frontiers in Psychology, 10, 1253. https://pmc.ncbi.nlm.nih.gov/articles/PMC6497769/
-
Lyons-Ruth, K. (2008). From infant attachment disorganization to adult dissociation: Relational adaptations or traumatic experiences? Psychiatric Clinics of North America, 29(1), 63–86. https://pmc.ncbi.nlm.nih.gov/articles/PMC2625289/
-
Corrigan, F. M., & Hull, A. M. (2024). The role of implicit memory in development and recovery from trauma-related disorders. Frontiers in Psychology, 15. https://pmc.ncbi.nlm.nih.gov/articles/PMC11523743/
Treatment and Intervention
-
Bakermans-Kranenburg, M. J., Van IJzendoorn, M. H., & Juffer, F. (2017). Disorganized infant attachment and preventive interventions: A review and meta-analysis. Infant Mental Health Journal, 26(3), 191–216. https://pubmed.ncbi.nlm.nih.gov/28397637/
-
Wright, B., & Edginton, E. (2016). Evidence-based parenting interventions to promote secure attachment: Decreasing rates of disorganised attachment. PLOS ONE, 11(7). https://journals.plos.org/plosone/article/file?type=printable&id=10.1371/journal.pone.0180858
Earned Security
- Roisman, G. I., Padrón, E., Sroufe, L. A., & Egeland, B. (2002). Earned-secure attachment status in retrospect and prospect. Child Development, 73(4), 1204–1219. https://pubmed.ncbi.nlm.nih.gov/12146743/
Comorbidity
-
Mosquera, D., Gonzalez, A., & Leeds, A. M. (2018). BPD as a generalization of disorganized attachment. Frontiers in Psychology, 9, 1962. https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2018.01962/full
-
BPD Foundation (2022). Dissociation in borderline personality disorder. https://bpdfoundation.org.au/
This article is for educational purposes only and is not a substitute for professional mental health treatment. If you are experiencing dissociation, trauma responses, or significant distress, please reach out to a licensed mental health professional who specializes in complex trauma and attachment.
