
Disorganized attachment can be healed. This attachment pattern—arising when a caregiver is simultaneously the source of safety and fear, creating what Main and Hesse (1990) called "fright without solution"—affects approximately 15 percent of children in normative samples and up to 23.5 percent across broader populations (van IJzendoorn et al., 1999). Research on earned secure attachment confirms that individuals with disorganized childhood attachment can develop secure patterns in adulthood (Filosa et al., 2024).
If you recognize this pattern in yourself, you already know why the question matters so deeply. Disorganized attachment is the style that often feels the most confusing and isolating—the push-pull of wanting closeness while fearing it. Healing is possible, but it typically requires more intensive, trauma-informed work than other insecure styles. This article is a research-grounded roadmap for what that process actually looks like.
Key takeaway: Disorganized attachment can be healed through trauma-informed therapy and body-based approaches. Research on earned secure attachment confirms that adults with disorganized childhood bonding can develop secure patterns. Healing requires addressing the cognitive, emotional, and somatic layers of the original wound, and typically involves longer-term, integrative treatment.
What Makes Disorganized Attachment Different From Other Insecure Styles?
If you carry this pattern, you may have noticed that your responses in relationships feel unpredictable even to you—drawn toward someone one moment, shutting down the next, without understanding why. That confusion makes sense. Disorganized attachment is unique because the attachment system receives contradictory signals—approach the caregiver for safety AND flee from them as the source of danger. The result is no coherent strategy for managing distress.
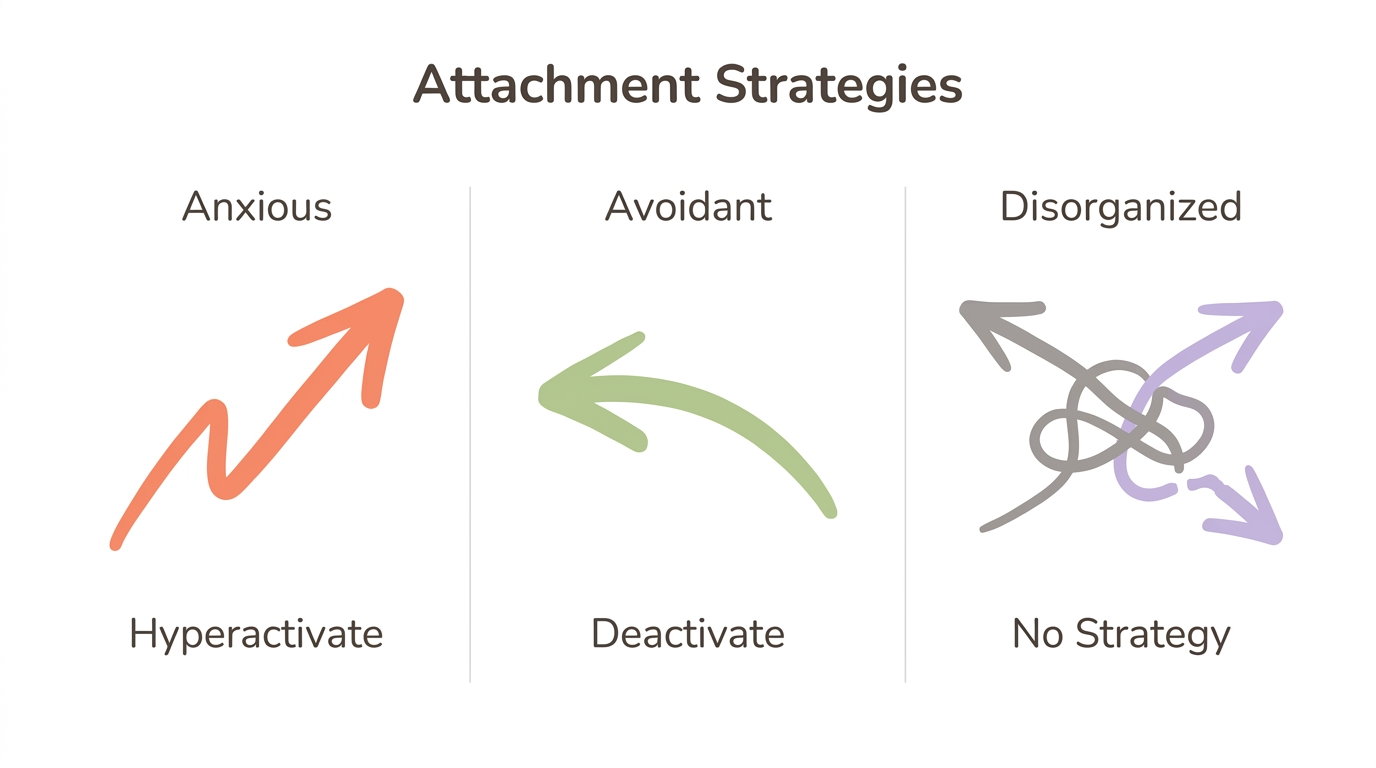
With anxious attachment, there is a clear (if exhausting) strategy: hyperactivate, pursue, seek reassurance. With avoidant attachment, the strategy is equally clear: deactivate, withdraw, suppress needs. Both are organized responses to an imperfect caregiving environment. Disorganized attachment has no such coherence. When the person who should make you feel safe is also the person who frightens you, your nervous system faces an impossible contradiction—and it collapses.
Main and Hesse (2000) described this as the caregiver being the simultaneous source of safety and fear. In their original research, parents classified as "unresolved" on the Adult Attachment Interview showed frightening or frightened behaviors toward their infants, and their children were overwhelmingly classified as disorganized. The prevalence of disorganized attachment rises dramatically in maltreatment samples—from approximately 15 percent in middle-class families to 45 to 48 percent among maltreated children (van IJzendoorn et al., 1999).
Understanding this distinction matters for healing. If you have a fearful-avoidant or disorganized pattern, generic attachment advice designed for anxious or avoidant styles will likely miss the mark. Your nervous system didn't learn a flawed strategy—it learned that no strategy works.
The Push-Pull Map (for disorganized attachment)
- Draw two columns on a page: "What makes me move toward people" and "What makes me pull away"
- List 5-7 entries in each column — be specific about people, situations, and feelings
- Circle any person or situation that appears in both columns
- Notice the overlap without judging it — this IS the contradictory activation that defines disorganized attachment
- Write one sentence about what you notice
This maps the collapsed strategy pattern that makes DA distinct. Seeing the contradiction on paper builds awareness — the first step toward choosing a response instead of being pulled in two directions simultaneously.
What Does the Research Actually Say About Healing Disorganized Attachment?
The research offers both genuine hope and important honesty. Earned secure attachment is real and achievable for individuals with disorganized childhood histories—but the evidence for specific interventions is more nuanced than most sources acknowledge.
A comprehensive scoping review by Filosa et al. (2024) confirmed that individuals with insecure childhood attachment—including disorganized—can develop secure attachment patterns in adulthood. Roisman et al. (2002) found that retrospectively defined earned-secures parent as effectively as continuous-secures, though they may carry residual depressive symptoms. This is meaningful: your history shapes you, but it does not define your ceiling.
The intervention research tells a more complex story. Bakermans-Kranenburg et al. (2005) conducted a meta-analysis of 15 preventive interventions across 842 families. The overall effect was non-significant (d = 0.05). However, sensitivity-focused interventions that began after six months of age showed significant effects (d = 0.23 to 0.24). Generic, broad-spectrum approaches did not move the needle—targeted ones did.
Latent class analysis by Fontana et al. (2016) revealed two distinct disorganized subclasses in adults, suggesting different levels of severity that may require different treatment approaches. This means "disorganized attachment" is not one monolithic experience—your specific presentation matters for choosing the right therapeutic path.
Three key research findings about healing disorganized attachment:
- Earned-secure individuals parent as effectively as those who were always securely attached (Roisman et al., 2002)—your children do not have to inherit your pattern
- Sensitivity-focused, targeted interventions produce measurable change (Bakermans-Kranenburg et al., 2005)—the type of intervention matters more than whether you get one at all
- Two disorganized subclasses exist in adults (Fontana et al., 2016)—severity and presentation differ, which means treatment should be tailored rather than one-size-fits-all
Coherent Narrative Journaling (for disorganized attachment)
- Set a timer for 10 minutes
- Write about one early caregiving memory — any memory that comes to mind
- Keep writing without editing or censoring
- When the timer ends, reread what you wrote
- Notice where you lost the thread, minimized, jumped topics, or went blank — mark these moments with a star
On the Adult Attachment Interview, disorganized/unresolved classification is marked by "lapses in monitoring of reasoning or discourse" when discussing loss or trauma. Those starred moments in your journaling mirror this pattern. The goal is not to write a perfect narrative — it is to notice where coherence breaks down, which is the first step toward building it.
Why Does Disorganized Attachment Feel So Hard to Heal?
Disorganized attachment presents three specific barriers to healing that other insecure styles do not face. Understanding these barriers is not discouraging—it is strategic. When you know what you are working with, you can choose approaches that actually match the challenge.
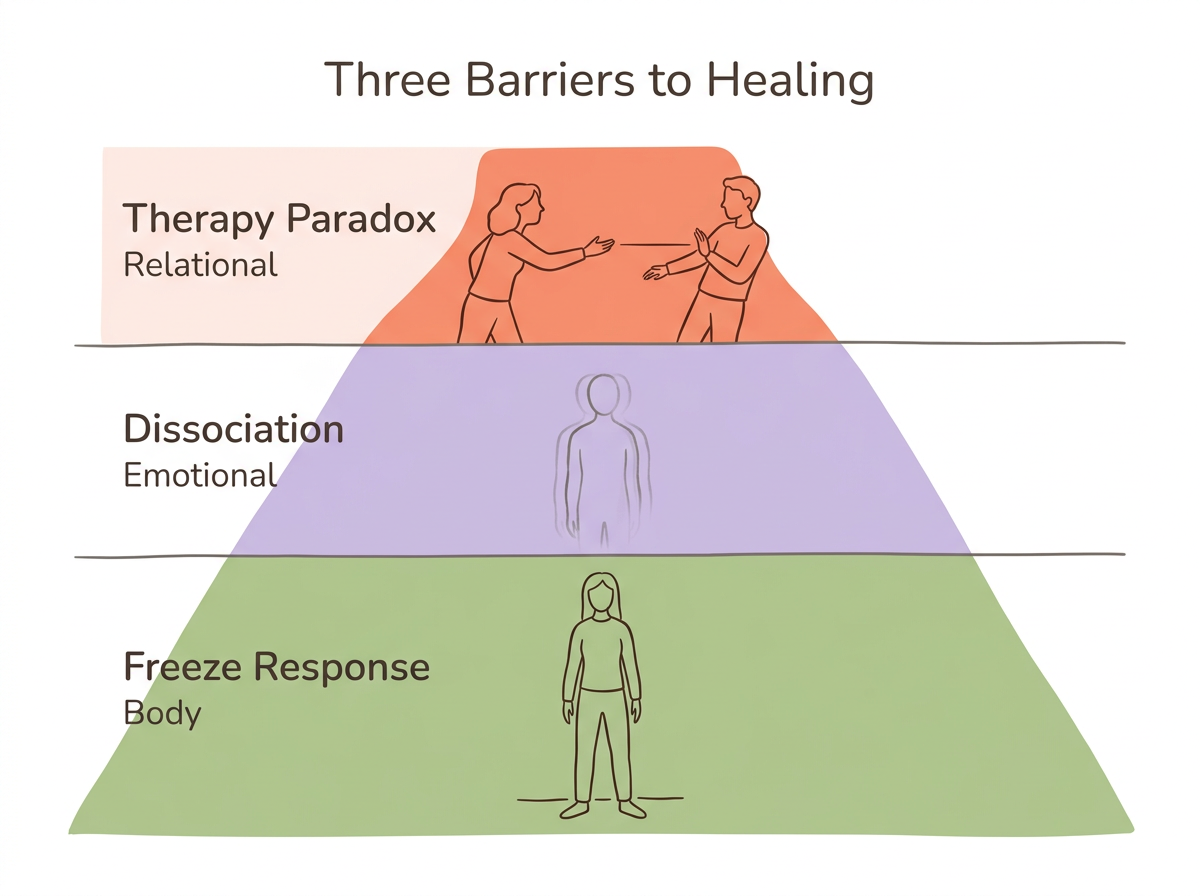
The Therapy Paradox
Your nervous system learned that caregiving figures are simultaneously needed and dangerous. Therapy asks you to trust a new caregiving figure—your therapist—which activates the exact wound. The consulting room recreates "fright without solution" at a neurobiological level. You may find yourself wanting to go to sessions and dreading them, opening up and then shutting down, trusting your therapist one week and doubting them the next. This is not resistance. This is your attachment system doing exactly what it learned to do.
Dissociation as a Barrier
Research links disorganized attachment strongly to borderline personality features, with individuals with BPD showing almost eight times higher odds of disorganized attachment (Frontiers in Psychology, 2018). Among BPD patients, 66 percent experience dissociation. You cannot process what you cannot stay present for. When emotions build in therapy or relationships, your nervous system may pull the emergency brake—going blank, numb, or "leaving" your body. This protective response made sense when the original threat was inescapable.
The Freeze Response Lives Below Cognition
Dorsal vagal collapse is a brainstem-level response, not a cognitive choice. When your nervous system detects a threat that cannot be fought or fled, the parasympathetic system over-regulates to the point of paralysis—the freeze or fawn response. Talk therapy alone often cannot reach patterns stored deeper than conscious thought, which is why body-based approaches are not optional for disorganized attachment. They are necessary.
Research on affective touch perception demonstrates how deeply this pattern lives in the body: individuals with disorganized attachment perceive gentle, caress-like touch as unpleasant, while those with organized attachment styles find the same touch pleasant (Scientific Reports, 2020). Your body literally interprets safety cues as threat cues.
5-4-3-2-1 Grounding for Dissociative Moments (somatic technique for disorganized attachment)
- When you notice yourself going blank, numb, or "leaving" during an emotional conversation, pause
- Name 5 things you can see — say them aloud if possible
- Touch 4 things within reach — notice their texture
- Identify 3 sounds you can hear right now
- Notice 2 things you can smell
- Name 1 thing you can taste
- Press your feet firmly into the floor and take 3 slow exhales, making the exhale longer than the inhale
Dissociation is the hallmark defensive response in disorganized attachment — the dorsal vagal system shuts you down when activation becomes overwhelming. This sequence engages your senses to bring the ventral vagal "social engagement" system back online, grounding you in the present moment rather than letting the nervous system collapse into shutdown.
What Happens in Your Brain and Body With Disorganized Attachment?
If your body seems to react before your mind can catch up—freezing mid-sentence, flinching at gentle touch, feeling simultaneously drawn to and terrified by closeness—there is a neurobiological reason for that. Disorganized attachment reshapes neural architecture, stress physiology, and even how your body interprets touch. Understanding these changes helps explain why healing requires more than insight alone—and why neuroplasticity means those changes are not permanent.
A 30-year longitudinal study found that children classified as disorganized at 18 months had a larger left amygdala volume in adulthood (Arancibia et al., 2023). The left amygdala develops more rapidly after birth and is especially responsive to maternal stimuli. When early caregiving was frightening, this threat-detection center grew larger and stayed on higher alert—a neural adaptation to an environment where danger came from the person meant to provide safety.
The same research found HPA axis dysregulation—mothers' cortisol levels predicted children's cortisol levels, which predicted compulsive behaviors and disorganized attachment classification. Your body learned to run on chronic stress activation because the environment demanded it.
Perhaps the most striking finding: individuals with disorganized attachment perceive gentle touch as unpleasant (Scientific Reports, 2020). The same caress-like stimulus that feels soothing to securely attached individuals registers as aversive in disorganized attachment. Your body encoded the approach-avoid conflict at the level of skin and nerve endings.
The mechanism that wired these patterns is the same one that can rewire them. Neuroplasticity works both ways. Consistent attunement from a therapist or partner, co-regulation practices, and somatic techniques that strengthen prefrontal cortex regulatory capacity can gradually shift the nervous system's baseline. Oxytocin—released through safe social bonding—helps calm the amygdala and reinforce relational security, creating a neurochemical foundation for earned secure attachment.
Safe Touch Recalibration (somatic/body-based technique for disorganized attachment)
- Sit comfortably and place one hand over your heart and one on your belly
- Apply gentle pressure — not too light, not too firm
- Notice what happens: does this feel calming, neutral, or uncomfortable?
- If uncomfortable, move your hands to your thighs, or hold a warm mug or a textured object instead
- Stay with whatever version feels most tolerable for 2 minutes
- Practice daily, noticing any shifts over time
This directly addresses the altered affective touch perception found in disorganized attachment research. Your body learned that gentle contact from a caregiver was unpredictable — sometimes soothing, sometimes frightening. Gradual self-administered touch at a tolerable intensity teaches the nervous system that contact can be safe, rebuilding the foundation that was disrupted.
What Therapy Is Best for Disorganized Attachment?
Integrative or sequential approaches work best for disorganized attachment because no single modality addresses all its dimensions. The cognitive, emotional, and somatic layers each need attention—and therapy for attachment change looks different for disorganized patterns than for anxious or avoidant ones.
| Therapy Type | What It Targets | Best For | Body-Based? | Evidence Level |
|---|---|---|---|---|
| EMDR | Fused trauma memories | Specific trauma processing | Partially | Strong (trauma) |
| IFS | Protective parts | Internal conflict | No | Growing |
| Somatic Experiencing | Freeze response | Body-level shutdown | Yes | Growing |
| EFT | Relationship cycles | Couples work | Partially | Strong (couples) |
| DBT | Emotional regulation | Distress tolerance | No | Strong (BPD) |
| ABFT | Family patterns | Intergenerational healing | No | Emerging |
-
EMDR (Eye Movement Desensitization and Reprocessing) targets the traumatic memories where love and fear were fused. Attachment-Focused EMDR integrates with IFS to address the protective parts that formed around those memories.
-
If you notice distinct "modes" in yourself—a part that clings, a part that shuts down, a part that rages—Internal Family Systems (IFS) offers a framework for working with those protective parts directly. IFS teaches these managers, firefighters, and exiles that they no longer need to run the show, creating internal safety before external relationships feel possible.
-
What does it feel like when your body goes into freeze during a conflict and no amount of reasoning brings you back? Somatic Experiencing (SE) works at precisely that level—the brainstem-stored collapse response that lives beneath the reach of language. SE helps the body complete the interrupted fight-or-flight responses that froze in place during childhood.
-
Emotionally Focused Therapy (EFT) maps and changes the negative interaction cycles that disorganized attachment creates in relationships. Particularly effective for couples where one or both partners carry disorganized patterns.
-
The oscillation between emotional flooding and total shutdown is one of the most exhausting features of disorganized attachment. DBT (Dialectical Behavior Therapy) builds concrete skills for riding that wave—distress tolerance, emotional regulation, and interpersonal effectiveness—providing a stabilizing foundation.
-
For adolescents and families, Attachment-Based Family Therapy (ABFT) works within the family system itself, repairing the ruptures between caregiver and child. It has shown effectiveness for adolescents with suicidality, depression, and trauma linked to attachment disruption.
Therapy Readiness Self-Assessment (for disorganized attachment) Rate yourself 1 to 5 on each question (1 = rarely, 5 = most of the time):
- Can I stay present during emotional conversations without going blank or numb?
- Do I feel safe enough with at least one person to be honest about my feelings?
- Can I notice when I am shutting down or dissociating?
- Am I willing to feel uncomfortable without leaving the situation?
If your total is 4 to 8: Consider starting with somatic or stabilization-focused work (SE, DBT skills) before trauma processing. If 9 to 15: You may be ready for integrative trauma work (EMDR, IFS). If 16 to 20: Relational approaches (EFT, exploratory therapy) may be a strong fit. This addresses the therapy paradox by matching you to the right starting point rather than diving into deep work before your nervous system can tolerate it.
Can You Heal Disorganized Attachment Without Therapy?
You can make meaningful progress without therapy, though professional support is strongly recommended for disorganized attachment given its trauma basis. Self-help alone is unlikely to be sufficient for most people with this pattern. That said, daily practices build the foundation that makes therapy more effective—and some healing happens outside the therapy room entirely.
Your nervous system learned its patterns in relationship, and earned security happens in relationship, not in isolation. Even one consistent, safe connection—a friend, partner, mentor, or community member—provides the co-regulation that gradually teaches your body a new template for what closeness can feel like.
Five practices that support healing between sessions:
-
Co-regulation with safe people — Identify one person whose presence helps your body settle. Spend regular, low-pressure time with them. Your nervous system needs repeated evidence that connection does not equal danger.
-
What are you feeling right now in your chest, your stomach, your jaw? If you are not sure, that is common with disorganized attachment. Interoception training through daily body scans—even 2 minutes—strengthens the prefrontal cortex's capacity to observe internal states before they escalate to shutdown.
-
Narrative coherence journaling — Writing about early experiences and noticing where the narrative breaks down builds the coherent story that the Adult Attachment Interview measures as "resolved."
-
Walking, yoga, and tai chi engage both sides of the body in rhythmic movement, similar to the bilateral stimulation used in EMDR. These bilateral body-based practices activate the ventral vagal system and help regulate the nervous system.
-
Sometimes the most powerful shift is recognizing "this is dorsal vagal shutdown, not weakness" or "this is a protective response, not a character flaw." Psychoeducation reduces shame and creates cognitive space between the trigger and your reaction. Articles like What Is Disorganized Attachment and How Does It Affect Relationships? and How to Develop Secure Attachment as an Adult can support this process.
Ventral Vagal Activation Sequence (somatic daily practice for disorganized attachment)
- Extended exhale breathing: Inhale through your nose for 4 counts, exhale slowly through your mouth for 6 counts. Repeat 5 rounds.
- Vocal vagus activation: Hum or sing gently for 30 seconds. The vibration of your vocal cords directly stimulates the vagus nerve.
- Slow lateral eye movements: Without moving your head, look slowly from left to right 5 times. This mimics the bilateral stimulation used in EMDR.
This three-step sequence targets the dorsal vagal shutdown that characterizes disorganized attachment by systematically activating the ventral vagal "social engagement" system. The extended exhale engages the parasympathetic brake, humming stimulates the vagus nerve directly, and lateral eye movements activate bilateral processing. Total time: approximately 3 minutes.
Am I Passing Disorganized Attachment to My Children?
This is one of the most painful questions a parent with disorganized attachment can ask. Your fear about repeating the cycle is itself evidence of the awareness that can break it.
Main and Hesse's research found that parents classified as "unresolved" on the Adult Attachment Interview were significantly more likely to have infants classified as disorganized—in their original sample, 11 of 12 unresolved mothers had disorganized infants (Hesse and Main, 2000). The intergenerational link is real. And it is not destiny.
Resolution of trauma breaks the cycle. Roisman et al. (2002) found that earned-secure parents parent as effectively as continuous-secure parents—those who were always securely attached. The mechanism is narrative coherence: making sense of your story so you do not unconsciously transmit unresolved fear through frightening or frightened behavior with your child (Filosa et al., 2024).
The Group Attachment-Based Intervention (GABI), developed by Anne Murphy with Miriam and Howard Steele, offers a group-based format specifically for parents with disorganized attachment histories. Programs like these demonstrate that the intergenerational transmission of disorganized attachment is a pattern, not a sentence—and patterns can be interrupted.
What matters is not being a perfect parent. What matters is being a parent who can notice ruptures and repair them—something that was missing in the original disorganized attachment experience.
The Repair Reflection (for parents with disorganized attachment) After a moment where you felt triggered or disconnected with your child:
- What happened? Write down the situation in 2-3 sentences
- What did I feel in my body? Note where tension, numbness, or activation showed up
- What old pattern got activated? Name it if you can — freeze, withdrawal, rage, collapse
- What would repair look like? Write one specific thing you could say or do
- If possible, do the repair — even something as simple as "I was upset earlier and I am sorry I got distant. That was about me, not about you."
This exercise targets the core of intergenerational transmission. Disorganized attachment develops when caregivers are frightening AND when ruptures go unrepaired. By naming what happened and offering repair, you model exactly what was missing in your own childhood — a caregiver who acknowledges disconnection and actively reconnects.
When Should You Seek Professional Help for Disorganized Attachment?
You should seek professional support if disorganized attachment patterns are significantly affecting your relationships, daily functioning, or emotional wellbeing. Seeking help is the secure behavior—it is the opposite of the "fright without solution" pattern. It is choosing "fright with solution."
Specific indicators that professional support is needed:
- Frequent dissociation—going blank, numb, or "leaving your body" during emotional conversations or conflict
- Repeating cycles of idealization and devaluation in relationships—intense connection followed by sudden withdrawal or hostility
- Inability to maintain relationships despite genuinely wanting them
- People-pleasing or fawning that leaves you feeling invisible in your own relationships
- Self-harm, suicidal ideation, or substance use to manage overwhelming emotional states
- Feeling "frozen" or paralyzed when conflict arises, unable to speak or think clearly
When choosing a therapist, look for someone trained in EMDR, IFS, Somatic Experiencing, or EFT who specifically understands attachment and complex trauma. Ask potential therapists: "What is your experience working with disorganized or fearful-avoidant attachment?" Their answer will tell you whether they understand the specific challenges this pattern presents.
If you are in crisis, contact the 988 Suicide and Crisis Lifeline (call or text 988) or the Crisis Text Line (text HOME to 741741).
Frequently Asked Questions
Can disorganized attachment be healed?
Yes. Research on earned secure attachment confirms that individuals with disorganized childhood attachment can develop secure patterns in adulthood through trauma-informed therapy. Healing requires addressing body-based and relational layers of the original wound, because disorganized attachment involves experiences where the caregiver was both safety and threat.
How long does it take to heal disorganized attachment?
Most clinicians estimate one to three years of consistent therapy, though meaningful shifts can begin within months. Disorganized attachment typically takes longer than anxious or avoidant healing because it involves the attachment and fear systems firing in opposition, requiring work at cognitive, emotional, and somatic levels.
What therapy is best for disorganized attachment?
Integrative approaches combining trauma processing like EMDR, parts work like IFS, and body-based methods like Somatic Experiencing show the most promise. No single modality addresses all dimensions of disorganized attachment—the cognitive, emotional, and somatic layers each need targeted attention.
Is disorganized attachment the same as fearful-avoidant?
They overlap significantly but come from different research traditions. Disorganized attachment is the developmental psychology term from Mary Main's infant classification system. Fearful-avoidant comes from Bartholomew's adult self-report model. Both describe the approach-avoid conflict, but disorganized emphasizes the trauma and collapse origin.
Is disorganized attachment linked to BPD?
Research shows individuals with BPD are almost eight times more likely to have disorganized attachment (Frontiers in Psychology, 2018). Both involve emotional dysregulation, identity instability, and fear of abandonment paired with fear of closeness. However, disorganized attachment does not inevitably lead to BPD—many individuals with this pattern never develop personality disorder criteria.
Why is disorganized attachment so hard to heal?
Three factors make it uniquely challenging: the therapeutic relationship itself triggers the approach-avoid wound, dissociation blocks emotional processing, and the freeze response is stored in the brainstem beneath the reach of language. Standard talk therapy alone often cannot access body-level patterns, which is why somatic approaches are especially important for disorganized attachment.
Can you have a healthy relationship with disorganized attachment?
Yes, though it requires self-awareness, communication about your patterns, and ideally therapeutic support. A partner who is consistently safe and responsive can serve as a co-regulating presence. Healing does not require perfection—it requires enough awareness to notice patterns and enough willingness to stay present through discomfort.
How do I stop dissociating in relationships?
Start with grounding techniques—the 5-4-3-2-1 sensory method, pressing feet into the floor, or holding ice. Build interoceptive awareness through daily body scans so you can catch dissociation earlier. Working with a trauma-informed therapist on underlying triggers addresses the root cause, since dissociation is the nervous system's protective response to perceived danger.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Foundational Works
-
Main, M., & Hesse, E. (1990). Parents' unresolved traumatic experiences are related to infant disorganized attachment status. In M. T. Greenberg, D. Cicchetti, & E. M. Cummings (Eds.), Attachment in the preschool years (pp. 161–182). University of Chicago Press.
-
Hesse, E., & Main, M. (2000). Disorganized infant, child, and adult attachment: Collapse in behavioral and attentional strategies. Journal of the American Psychoanalytic Association, 48(4), 1097–1127.
-
van IJzendoorn, M. H., Schuengel, C., & Bakermans-Kranenburg, M. J. (1999). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11(2), 225–250.
Earned Security and Healing Evidence
-
Filosa, M., et al. (2024). Earned secure attachment: A scoping review. Psychological Reports.
-
Roisman, G. I., Padrón, E., Sroufe, L. A., & Egeland, B. (2002). Earned-secure attachment status in retrospect and prospect. Child Development, 73(4), 1204–1219.
-
Bakermans-Kranenburg, M. J., van IJzendoorn, M. H., & Juffer, F. (2005). Disorganized infant attachment and preventive interventions: A review and meta-analysis. Infant Mental Health Journal, 26(3), 191–216.
Neuroscience
-
Arancibia, M., et al. (2023). Neurobiology of disorganized attachment: A review. Neuroscience Insights.
-
Lucarini, V., et al. (2020). Affective touch perception in disorganized attachment. Scientific Reports, 10, 9658.
-
Feldman, R. (2017). The neurobiology of human attachments. Trends in Cognitive Sciences, 21(2), 80–99.
Clinical Subtypes and Comorbidity
-
Fontana, A., et al. (2016). Disorganized attachment and personality functioning: A latent class analysis. Personality Disorders: Theory, Research, and Treatment, 7(3), 260–269.
-
Choi-Kain, L. W., Fitzmaurice, G. M., Zanarini, M. C., Laverdière, O., & Bhawan, J. (2018). BPD as a generalization of disorganized attachment. Frontiers in Psychology, 9, 1962.
-
Bakkum, L., et al. (2023). Unresolved classification in the Adult Attachment Interview. Attachment & Human Development, 25(4).
-
Exploring unresolved loss in 1,000+ Adult Attachment Interviews. (2023). Attachment & Human Development.
Therapeutic Approaches
-
Diamond, G. S., et al. (2021). Attachment-Based Family Therapy: Theory, model, and outcomes. PMC.
-
EMDRIA. EMDR therapy and Internal Family Systems (IFS).
-
Leading Edge Seminars. Polyvagal theory in therapy: Attachment and trauma.
-
Murphy, A., Steele, H., & Steele, M. Group Attachment-Based Intervention (GABI). Center for Attachment Research.
Polyvagal Theory and Somatic Approaches
-
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
-
Graham, L. (2013). Bouncing back: Rewiring your brain for maximum resilience and well-being. New World Library.
-
Levine, P. A. (2010). In an unspoken voice: How the body releases trauma and restores goodness. North Atlantic Books.
This article is for educational purposes only and is not a substitute for professional mental health treatment. Disorganized attachment patterns are rooted in early relational trauma, and healing typically benefits from the support of a licensed therapist trained in attachment and complex trauma. If you are in crisis, please contact the 988 Suicide and Crisis Lifeline (call or text 988) or the Crisis Text Line (text HOME to 741741).
