
Avoidant attachment is a relational pattern defined by the systematic deactivation of attachment needs—suppressing vulnerability, distancing from closeness, and relying on self-sufficiency to avoid anticipated rejection. If you tend to pull away when people get close—even when part of you wants connection—you may recognize this pattern. Approximately 22 to 25 percent of adults have avoidant attachment (Mickelson et al., 1997), and dismissive attachment in American college students rose from roughly 12 percent to 19 percent between 1988 and 2011 (Konrath et al.).
Here is the paradox: the people who could benefit most from therapy are often the least likely to seek it—and the most likely to leave early. If you recognize avoidant patterns in yourself, this guide covers which therapies have the strongest evidence for avoidant attachment specifically, what to expect in session, and how to choose an approach that works with your nervous system rather than against it.
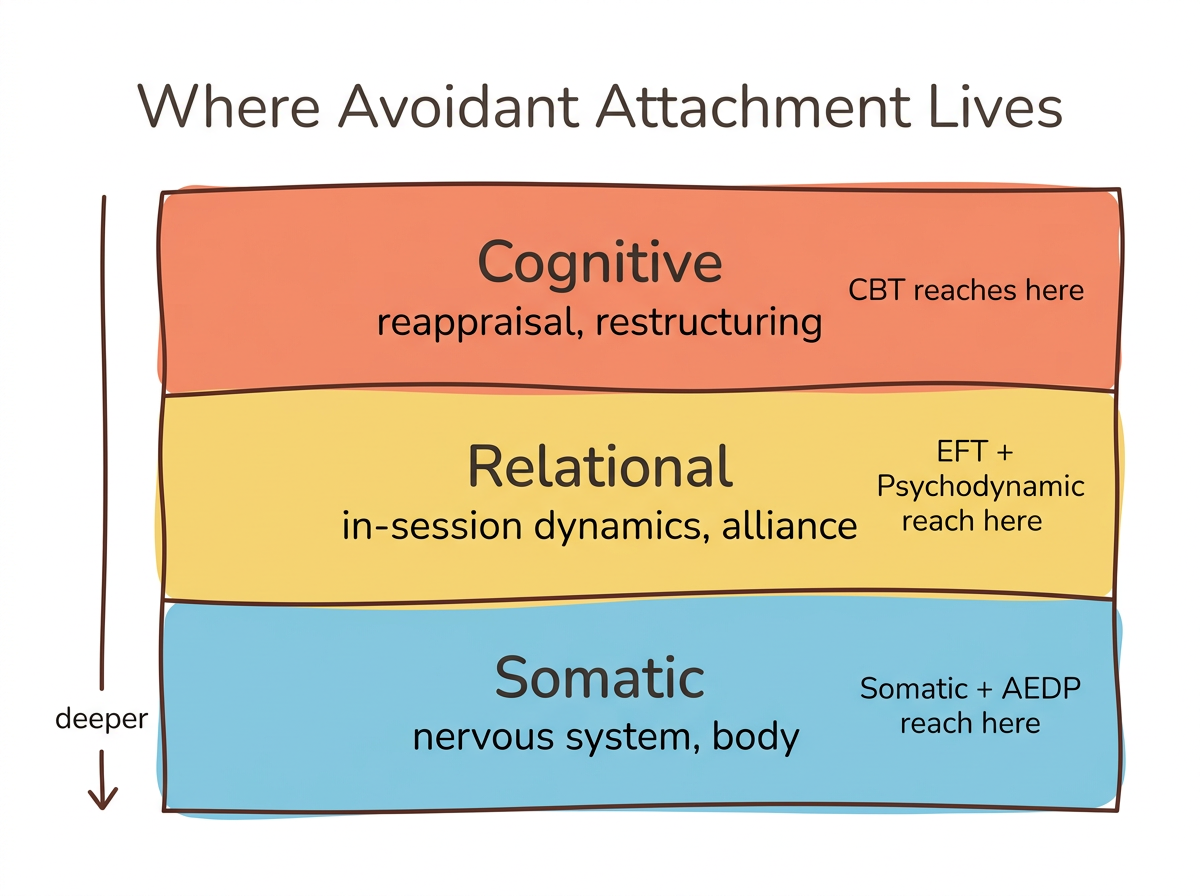
Key takeaway: Research-supported therapies for avoidant attachment include emotionally focused therapy, psychodynamic therapy, and CBT with emotional processing components. Because avoidant patterns involve suppressing emotions rather than reappraising them, effective therapy must go beyond cognitive techniques to include emotional processing and body-based work. The therapeutic relationship itself becomes the primary vehicle for change.
Why Is Avoidant Attachment So Hard to Treat?
Avoidant attachment is difficult to treat because the core protective strategy—deactivating the attachment system—directly conflicts with what therapy requires: emotional openness, vulnerability, and relational trust. Mikulincer and Shaver (2003, 2007) describe deactivating strategies as a coordinated system of suppressing attachment needs, cognitively distancing from emotional threats, repressing painful memories, and redirecting attention away from attachment-related cues.
These strategies create a specific challenge in the therapy room. Meta-analyses show small but significant negative correlations (r = -.12 to -.17) between attachment avoidance and therapeutic working alliance (Diener and Monroe, 2011). Your therapist may feel kept at arm's length—because your nervous system is doing exactly what it learned to do.
Avoidant attachment is also a risk factor for premature dropout from therapy. The urge to quit after a few sessions—telling yourself "this isn't working" or "I don't need this"—is not a sign that therapy is wrong for you. That urge is the deactivating strategy doing its job. Recognizing this pattern is the first step toward staying long enough for therapy to work.
Research also confirms that alliance strength improves significantly over time even for avoidant clients when the therapist maintains consistency. The difficulty is at the beginning, not the end. If you are wondering whether avoidant attachment can be healed, the answer is yes—but it requires understanding why the first few weeks feel so uncomfortable.
The Deactivation Tracker (for dismissive-avoidant awareness)
Keep a small notebook or notes app open for one week. Each evening, scan your day for moments when you pulled away, intellectualized, or felt "nothing" during a relational moment. For each one, jot down three things: what happened, what you did (pulled away, changed the subject, went blank), and what you might have been feeling underneath—even a guess counts.
At the end of the week, look for patterns. When does deactivation show up most? With whom? The goal is not to change anything yet—just to notice. Your nervous system clears emotional data quickly, and this exercise captures it before it disappears, targeting the tendency to arrive at therapy with "nothing to talk about."
Why Doesn't Standard CBT Work Well Enough for Avoidant Attachment?
Standard CBT alone often falls short for avoidant attachment because it relies heavily on cognitive reappraisal—and neuroscience shows reappraisal fails to reduce amygdala activation in avoidant individuals. Vrtička et al. (2012) found that when securely attached people used cognitive reappraisal to manage negative social images, their amygdala calmed down. When avoidant individuals tried the same strategy, their amygdala stayed activated. Avoidant individuals preferentially rely on suppression over reappraisal—pushing emotions down rather than reframing them.
The takeaway is not that cognitive approaches are useless—it is that emotional processing must be added. Newman et al. (2015) conducted an RCT with 83 participants with generalized anxiety disorder and found that higher dismissing attachment predicted greater symptom improvement in CBT combined with interpersonal and emotional processing (CBT+I/EP), with an effect size of d = -0.56 maintained at two-year follow-up. The same dismissing attachment did not predict improvement in CBT with supportive listening alone.
Three reasons standard CBT alone falls short for avoidant clients:
- Reappraisal bypasses the real issue. Avoidant nervous systems are already efficient at cognitive override—reappraisal asks them to do more of what they already do.
- Relational patterns stay untouched. Standard CBT targets thoughts and behaviors but often does not address the in-session relational dynamics where avoidant patterns play out in real time.
- The body is left out. Avoidant attachment lives in the nervous system—numbness, tension, emotional flatness. Cognitive techniques alone do not reach the somatic layer where attachment patterns are stored.
Which Therapies Have the Strongest Evidence for Avoidant Attachment?
Three therapeutic modalities have the most direct research support for shifting avoidant attachment toward earned security: emotionally focused therapy, psychodynamic/transference-focused therapy, and CBT with interpersonal emotional processing.
Emotionally Focused Therapy (EFT)
Wiebe et al. (2016) reviewed the EFT research base and found that EFT significantly reduced avoidant attachment and increased secure attachment in experimental versus control groups. Decreases in attachment avoidance were the strongest predictor of higher relationship satisfaction at follow-up. The key mechanism for avoidant clients is accessing the vulnerability that lives beneath the withdrawal pattern.
Your nervous system learned to shut down for good reason. EFT does not try to override that protection—it creates enough safety that you can explore what is underneath it at your own pace.
One important finding deserves attention: avoidant clients in EFT may experience a temporary "shame spike"—an increase in shame that can feel alarming but actually reflects growing emotional awareness, not a setback. When you have spent years keeping feelings at a distance, feeling shame means your emotional system is coming back online.
Adaptation matters here. Jorgensen's clinical work shows that avoidant partners need slower emotional deepening and more emphasis on safety before vulnerability is invited. A skilled EFT therapist will not push you to "go deep" in session three.
Psychodynamic and Transference-Focused Therapy (TFP)
Levy et al. (2006) conducted the most rigorous RCT on attachment change in therapy. Ninety patients with borderline personality disorder were randomized to transference-focused therapy, dialectical behavior therapy, or supportive psychotherapy for 12 months. Only TFP produced significant increases in secure attachment classification and reflective function. Neither DBT nor supportive therapy moved the needle on attachment.
TFP works by integrating polarized representations of self and other. If your internal model says "people will reject me if I show need," TFP uses the therapeutic relationship to gradually disconfirm that expectation. The therapist's consistent, attuned presence becomes a corrective attachment experience.
Long-term psychodynamic work has produced striking individual results. Callahan and Hilsenroth (2016) documented a woman with avoidant attachment and avoidant personality disorder who achieved earned-secure attachment and full symptom remission through psychodynamic therapy, published in the American Journal of Psychotherapy.
CBT with Interpersonal and Emotional Processing
Newman et al. (2015) demonstrated that avoidant clients benefited more from structured therapy that specifically targeted emotion and relationships. In their RCT, higher dismissing attachment predicted greater GAD symptom change in CBT combined with interpersonal/emotional processing (d = -0.56) but not in CBT with supportive listening. This effect held at two-year follow-up (d = -0.53).
The implication is clear: cognitive restructuring alone is not enough for avoidant attachment. When emotional processing and relational focus are woven into the cognitive framework, avoidant clients respond well—sometimes better than other attachment styles.
Naming the Withdrawal (in-session communication tool for dismissive-avoidant clients)
Before your next therapy session, choose a simple signal for when you notice yourself shutting down—raising a hand, touching your collarbone, or saying a phrase like "I think I'm shutting down right now."
When you notice going blank, intellectualizing, or wanting to change the subject mid-session, use your signal. You do not need to know why you are shutting down—just naming it is enough. Then notice what happens in your body when you name the withdrawal instead of acting on it.
This targets the dismissive-avoidant tendency to dissociate without awareness, building interoceptive capacity within the safety of the therapeutic relationship. Naming the deactivation interrupts it just enough to create a choice point—and choice is where change begins.
What About Schema Therapy, IFS, and EMDR for Avoidant Attachment?
Several emerging modalities show strong theoretical fit for avoidant attachment, though with less RCT evidence than EFT or psychodynamic approaches. Each addresses avoidant patterns through a different lens—and one may resonate more with your particular experience.
Schema Therapy
Schema therapy targets the early maladaptive schemas most linked to avoidant attachment: emotional inhibition, defectiveness and shame, emotional deprivation, and mistrust. These schemas formed early—before you had language for them—and they operate automatically in adult relationships.
The technique of limited reparenting within schema therapy provides a corrective emotional experience. The therapist meets the unmet needs that the original caregiving environment could not provide, within appropriate therapeutic boundaries. More rigorous effectiveness studies specifically for avoidant attachment are still needed, but the theoretical alignment is strong.
Internal Family Systems (IFS)
IFS offers a framework that many avoidant readers find immediately recognizable. Your self-reliance is not all of you—it is a part of you. In IFS language, protector parts (managers) learned to dismiss your needs for closeness to anticipate and prevent rejection. Exiles carry the original pain of those unmet attachment needs—the loneliness, the longing, the grief.
The therapeutic approach is to befriend protectors rather than force vulnerability. A skilled IFS therapist will not try to bypass your defensive parts. Instead, they help you understand why those parts developed, building trust gradually until the exiles can be accessed safely. No RCTs exist specifically for IFS and avoidant attachment, but clinical literature is growing.
For readers curious about disorganized or fearful-avoidant patterns, IFS also addresses the more complex push-pull dynamics where avoidant and anxious strategies alternate.
Attachment-Focused EMDR (AF-EMDR)
Parnell (2008) developed AF-EMDR to address limitations of standard EMDR for attachment-based trauma. Rather than processing single traumatic events, AF-EMDR works with the relational wounds that shaped your attachment system. Wesselmann and Potter (2009) documented three case studies showing movement from insecure or disorganized toward more secure attachment classification post-treatment.
One critical caveat: rushing EMDR processing triggers deactivation in avoidant clients. The rapport-building phase takes longer, and a therapist experienced with avoidant attachment will honor that timeline rather than pushing into processing prematurely.
Parts Mapping (IFS-informed self-exploration for avoidant readers)
Think of one recent situation where you pulled away from closeness—canceled plans, went quiet, felt "nothing" when a partner expressed emotion. Then sit with these reflection questions, one at a time:
- What part of me pulled away? Does it have a name, an image, an age?
- What is that part protecting me from? (Rejection? Being seen? Losing control? Disappointment?)
- How old does that protective instinct feel? When did it first learn to do this?
- What would that part need to hear to feel safe enough to soften—even slightly?
This targets the dismissive-avoidant pattern of treating self-reliance as identity rather than strategy. Avoidance is a part of you—a loyal, hard-working part—not the whole of who you are. Separating "I am avoidant" from "a part of me avoids" creates space for other parts to emerge.
How Can Somatic and Body-Based Approaches Help Avoidant Attachment?
Picture this: a client sits across from their therapist, asked "How does that make you feel?" and genuinely cannot answer—not because they are withholding, but because the signal between body and brain has been muted for years. Through a polyvagal lens, avoidant attachment maps onto dorsal vagal shutdown (Porges): the numbness, disconnection, and emotional flatness that show up when intimacy is invited. Somatic approaches work directly with the nervous system rather than trying to think through patterns that live in the body, bypassing the cognitive suppression that avoidant individuals rely on.
That flatness is not indifference. It is your body's version of deactivation—a protective response your nervous system learned when closeness felt unsafe. Vrtička et al. (2008) found that avoidant attachment correlated with reduced ventral striatum and VTA activation to positive social feedback—meaning social rewards literally register less in the brain. Vrtička et al. (2012) also showed increased cognitive control recruitment in avoidant individuals, with heightened activation in medial prefrontal cortex, precuneus, and dorsolateral PFC—cognitive control areas working overtime to suppress emotional responses.
Bottom-up approaches like somatic experiencing and body-based therapies sidestep this effortful suppression entirely. Rather than asking you to talk about your feelings—which activates the same cognitive control loop—somatic work invites you to notice what is happening in your body without narrating or analyzing it.
AEDP (Accelerated Experiential Dynamic Psychotherapy) combines somatic awareness with relational depth. Explicitly designed for attachment wounds, AEDP uses "recognition sequences" between therapist and client to target the chronic emptiness and disconnection that avoidant individuals often describe. Understanding your window of tolerance provides a framework for recognizing when your body drops into shutdown.
Container and Contact (somatic awareness practice for dismissive-avoidant readers)
Sit comfortably and place one hand on your chest, one on your belly. Take three slow breaths—inhale for 4 counts, exhale for 6 counts. Now imagine someone you care about sitting next to you and placing their hand gently on your shoulder.
What happens? Where do you feel tension? Numbness? A pulling-away sensation? Warmth? Rate the intensity on a scale of 1 to 10. Practice for 60 seconds daily, gradually increasing to 3 minutes over several weeks.
Sensation Where in your body? Intensity (1–10) Tension Numbness Warmth Pulling away Other: ___ This targets the dorsal vagal shutdown pattern by building tolerance for proximity sensations without requiring verbal vulnerability. You are not being asked to talk about feelings—you are being asked to notice your body's response to imagined closeness. That distinction matters for avoidant nervous systems, because it engages the ventral vagal pathway without triggering the cognitive suppression loop.
What Should You Look for in a Therapist If You Have Avoidant Attachment?
Finding the right therapist matters more for avoidant clients than almost any other attachment style—because your pattern is designed to find reasons to leave. Look for a therapist trained in attachment theory, emotionally focused therapy, or psychodynamic approaches who is comfortable with silence and understands that trust builds slowly.
Your pattern tells you that people will eventually demand more than you can give. A good therapist will disconfirm that expectation by not pushing vulnerability too fast and not interpreting your guardedness as resistance. What progress looks like for avoidant clients is often subtle—noticing emotions before they have already passed, tolerating five more seconds of eye contact, feeling a flicker of sadness where you used to feel nothing.
Five questions to ask a potential therapist during a consultation call:
- "What is your approach to working with clients who tend to shut down emotionally?"
- "How do you handle it when a client wants to quit therapy?"
- "Do you have training in attachment theory or emotionally focused approaches?"
- "Are you comfortable with silence in sessions, or do you tend to fill it?"
- "How do you think about the pace of emotional work—do you follow the client's timeline?"
Commit to a minimum number of sessions. Research shows the therapeutic alliance improves significantly over time even for avoidant clients when the therapist maintains consistency. Consider committing to at least 10 to 12 sessions before evaluating whether therapy is "working." The urge to leave at session four is the pattern talking—not your judgment.
If you are in a relationship with an anxiously attached partner, couples therapy with an EFT-trained therapist can address the pursue-withdraw cycle directly rather than through individual work alone.
Pre-Session Intention Setting (behavioral commitment tool for avoidant readers starting therapy)
Before each therapy session, finish this sentence: "One thing I noticed this week that I would normally keep to myself is ___."
It can be small—a moment of irritation, a flicker of loneliness, a time you almost reached out to someone but did not. If nothing comes to mind, write: "I noticed myself feeling nothing, and that itself is worth mentioning." Bring it to session. You do not have to share it—but having it written gives you the option.
This targets the dismissive-avoidant pattern of arriving at sessions with nothing to discuss. Your deactivating strategies clear emotional data efficiently—this exercise captures experiences before they disappear, giving your therapist something real to work with.
Therapy Approaches for Avoidant Attachment: Evidence and Fit
| Therapy | Best For | Key Mechanism | Evidence Level | Typical Duration | Body-Based Component |
|---|---|---|---|---|---|
| EFT | Dismissive-avoidant in couples; emerging for individual | Accessing vulnerability beneath withdrawal | RCT-supported reviews | 12–20 sessions (couples) | Partial |
| Psychodynamic/TFP | Dismissive-avoidant seeking deep relational change | Corrective attachment experience via therapeutic relationship | RCT (Levy et al., 2006) | 1–3 years | No |
| CBT + Emotional Processing | Dismissive-avoidant with anxiety or structured-learning preference | Adding emotional and relational processing to cognitive work | RCT (Newman et al., 2015) | 16–24 sessions | No |
| Schema Therapy | Avoidant with early maladaptive schemas (shame, deprivation) | Limited reparenting and schema restructuring | Clinical studies | 1–2 years | Partial |
| IFS | Avoidant wanting to understand protective parts | Befriending protectors rather than forcing vulnerability | Clinical literature | Variable | Partial |
| AF-EMDR | Avoidant with attachment-related trauma memories | Bilateral processing of relational wounds | Case studies | 12–24 sessions | Yes |
| Somatic/AEDP | Avoidant experiencing numbness, emotional flatness, shutdown | Bypassing cognitive suppression via body awareness | Clinical literature | Variable | Yes |
When Should You Seek Professional Help for Avoidant Attachment?
Seeking therapy for avoidant attachment is an act of proactive growth, not crisis intervention. None of this requires waiting until everything falls apart. That said, several patterns suggest it is time.
Consider reaching out if you notice multiple relationships ending the same way—partners telling you they feel shut out, friendships fading because you never initiate, a chronic sense that you are watching your life from behind glass. Persistent emotional numbness, feedback from more than one person that you are "hard to reach," or wanting closeness but having no idea how to sustain it are all signals that your deactivating strategies are costing you something you value.
Many avoidant clients enter therapy for reasons that seem unrelated—work stress, general anxiety, insomnia, a partner's ultimatum—and discover their attachment patterns along the way. That is a perfectly valid entry point. There is no requirement to arrive with the words "avoidant attachment" already in your vocabulary.
If you are pushing people away while wanting them close or wondering whether this is a trauma response, those questions are worth exploring with a professional who understands attachment dynamics.
Between sessions, tools like the Meadow app can help you track your patterns, build emotional vocabulary, and practice the micro-moments of awareness that add up to real change over time. You do not rewire attachment in a single insight. You rewire it by noticing 10 percent earlier, responding 10 percent differently, 10 percent more often.
Frequently Asked Questions
Can avoidant attachment be fixed with therapy?
Yes. Research shows therapy can shift avoidant attachment toward earned security. Levy et al.'s RCT found transference-focused therapy moved clients from insecure to secure classification in 12 months. The therapeutic relationship provides a corrective attachment experience that gradually disconfirms expectations of rejection.
What is the best therapy for dismissive avoidant specifically?
EFT and psychodynamic therapy have the strongest evidence. EFT accesses vulnerability beneath withdrawal patterns, while psychodynamic work uses the therapeutic relationship to integrate polarized self-other representations. Both require patience—dismissive-avoidant clients need slower emotional deepening and more safety before vulnerability.
How long does therapy for avoidant attachment take?
Most attachment-focused therapy requires six to twelve months minimum to see meaningful shifts, with deeper change often emerging over one to two years. Short-term protocols of 12 to 20 sessions can build awareness and skills, but rewiring deeply ingrained deactivating strategies typically requires longer-term relational work. How long does it take to change your attachment style? covers realistic timelines.
Why is it hard for avoidant people to go to therapy?
Avoidant attachment involves systematically suppressing attachment needs—and therapy requires activating those same needs. The therapeutic relationship triggers the avoidant system: closeness feels threatening, vulnerability feels dangerous. Meta-analyses confirm avoidant attachment correlates with weaker working alliance and higher dropout risk (Diener and Monroe, 2011).
Can EMDR help avoidant attachment?
Attachment-Focused EMDR, developed by Laurel Parnell, adapts standard EMDR for attachment wounds. Case studies by Wesselmann and Potter (2009) show movement toward more secure attachment post-treatment. The rapport-building phase takes longer with avoidant clients because rushing processing can trigger deactivation and shutdown.
Is CBT or psychodynamic therapy better for avoidant attachment?
Standard CBT alone may be insufficient—neuroscience shows cognitive reappraisal fails to reduce amygdala activation in avoidant individuals (Vrtička et al., 2012). CBT with added emotional processing components shows strong results (Newman et al., 2015). Psychodynamic therapy has direct RCT evidence for attachment change. The best choice depends on your comfort level, goals, and available therapists.
What does therapy for avoidant attachment look like session by session?
Early sessions focus on safety and alliance-building—expect to feel guarded, and know that guardedness is normal and expected. Middle sessions explore emotional patterns and relational dynamics. Later sessions practice vulnerability with the therapist. Progress feels subtle: noticing emotions before they pass or tolerating closeness slightly longer.
How do I find a therapist who understands avoidant attachment?
Look for therapists trained in EFT, attachment theory, or psychodynamic approaches. During consultation, ask how they work with clients who shut down emotionally and whether they are comfortable with silence. A therapist who does not push vulnerability too fast signals good fit.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
RCTs and Meta-Analyses
-
Levy, K. N., Meehan, K. B., Kelly, K. M., Reynoso, J. S., Weber, M., Clarkin, J. F., & Kernberg, O. F. (2006). Change in attachment patterns and reflective function in a randomized control trial of transference-focused psychotherapy for borderline personality disorder. Journal of Consulting and Clinical Psychology, 74(6), 1027–1040.
-
Newman, M. G., Castonguay, L. G., Jacobson, N. C., & Moore, G. A. (2015). Adult attachment as a moderator of treatment outcome for generalized anxiety disorder: Comparison between cognitive-behavioral therapy (CBT) plus interpersonal and emotional processing therapy (I/EP) and CBT plus supportive listening. Journal of Consulting and Clinical Psychology, 83(5), 915–925.
-
Wiebe, S. A., Johnson, S. M., Lafontaine, M. F., Burgess Moser, M., Dalgleish, T. L., & Tasca, G. A. (2016). Two-year follow-up outcomes in emotionally focused couple therapy: An investigation of relationship satisfaction and attachment trajectories. Journal of Marital and Family Therapy, 43(2), 227–244.
-
Diener, M. J., & Monroe, J. M. (2011). The relationship between adult attachment style and therapeutic alliance in individual psychotherapy: A meta-analytic review. Psychotherapy, 48(3), 237–248.
-
Bernecker, S. L., Levy, K. N., & Ellison, W. D. (2014). A meta-analysis of the relation between patient adult attachment style and the working alliance. Psychotherapy Research, 24(1), 12–25.
-
van IJzendoorn, M. H., & Kroonenberg, P. M. Cross-cultural patterns of attachment: A meta-analysis of the Strange Situation. Child Development.
Neuroscience
-
Vrtička, P., Andersson, F., Grandjean, D., Sander, D., & Vuilleumier, P. (2008). Individual attachment style modulates human amygdala and striatum activation during social appraisal. PLoS ONE, 3(8), e2868.
-
Vrtička, P., Bondolfi, G., Sander, D., & Vuilleumier, P. (2012). The neural substrates of social emotion perception and regulation are modulated by adult attachment style. Social Neuroscience, 7(5), 473–493.
-
DeWall, C. N., Masten, C. L., Powell, C., Combs, D., Schurtz, D. R., & Eisenberger, N. I. (2011). Do neural responses to rejection depend on attachment style? An fMRI study. Social Cognitive and Affective Neuroscience, 7(2), 184–192.
Attachment Theory
-
Mikulincer, M., & Shaver, P. R. (2003). The attachment behavioral system in adulthood: Activation, psychodynamics, and interpersonal processes. Advances in Experimental Social Psychology, 35, 53–152.
-
Mikulincer, M., & Shaver, P. R. (2007). Attachment in adulthood: Structure, dynamics, and change. Guilford Press.
-
Mickelson, K. D., Kessler, R. C., & Shaver, P. R. (1997). Adult attachment in a nationally representative sample. Journal of Personality and Social Psychology, 73(5), 1092–1106.
Clinical Approaches
-
Callahan, J. L., & Hilsenroth, M. J. (2016). Earned-secure attachment in psychotherapy: A case study. American Journal of Psychotherapy, 70(3), 233–254.
-
Parnell, L. (2008). Tapping in: A step-by-step guide to activating your healing resources through bilateral stimulation. Sounds True.
-
Wesselmann, D., & Potter, A. E. (2009). Change in adult attachment status following treatment with EMDR: Three case studies. Journal of EMDR Practice and Research, 3(3), 178–186.
-
Jorgensen, R. Adapting EFT to attachment styles in couples therapy. Clinical practice paper.
Polyvagal and Somatic
- Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
Prevalence and Trends
- Konrath, S. H., Chopik, W. J., Hsing, C. K., & O'Brien, E. (2014). Changes in adult attachment styles in American college students over time: A meta-analysis. Personality and Social Psychology Review, 18(4), 326–348.
This article is for educational purposes only and is not a substitute for professional mental health treatment. If you are experiencing significant distress related to your attachment patterns, please consult a licensed therapist or counselor who specializes in attachment-focused approaches.
